For curriculum alignment and exam blueprint context, see Royal College of Emergency Medicine and explore learning resources via RCEMLearning.
this picture Illustration is from "rcem eLearning "
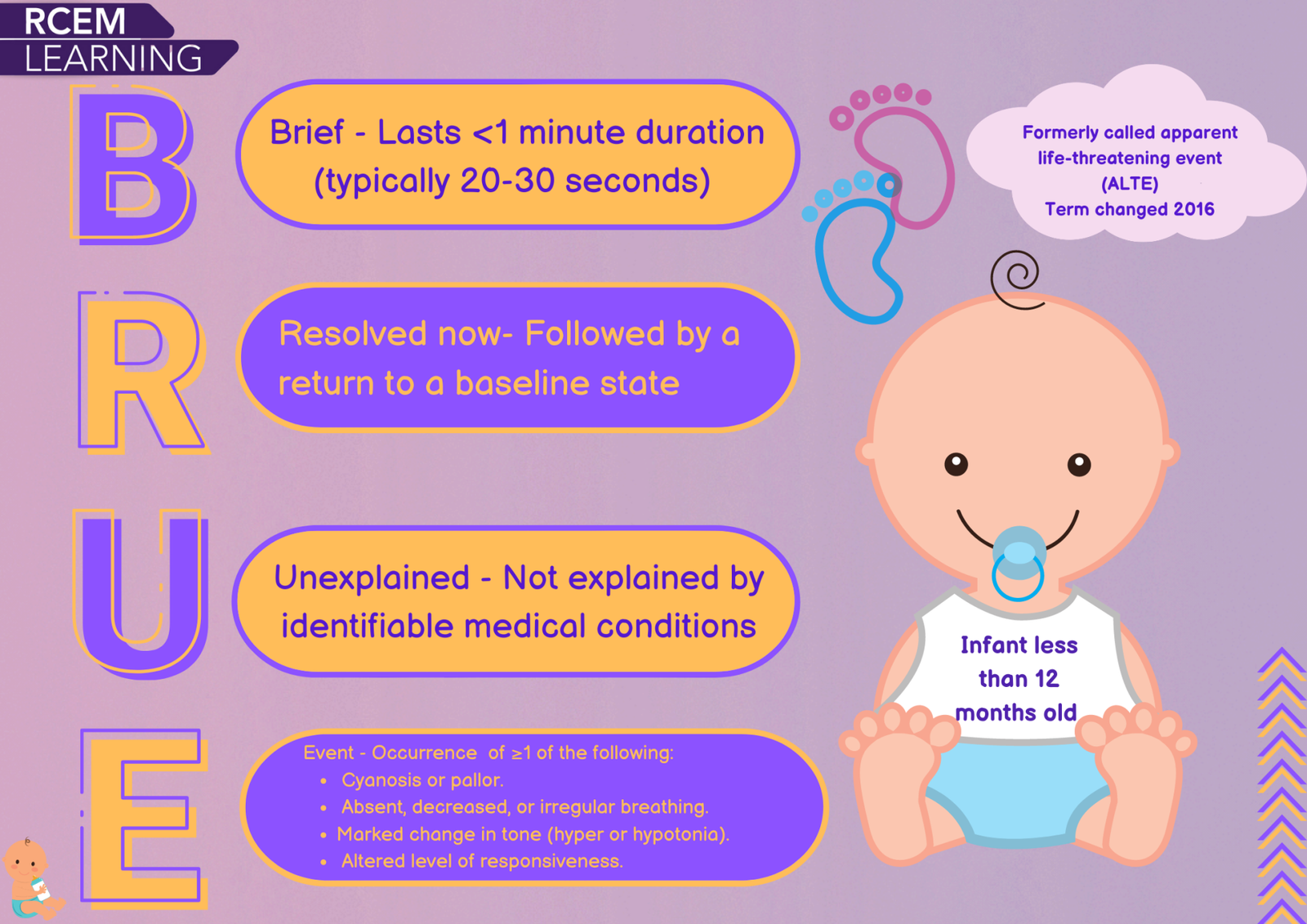
A BRUE is an event in an infant <12 months that:
Key Principle: BRUE is a diagnosis of exclusion—not a disease entity.
BRUE SBAs assess:
High scorers apply criteria strictly and avoid premature closure.
Systematically consider:
If a cause is identified, it is not BRUE.
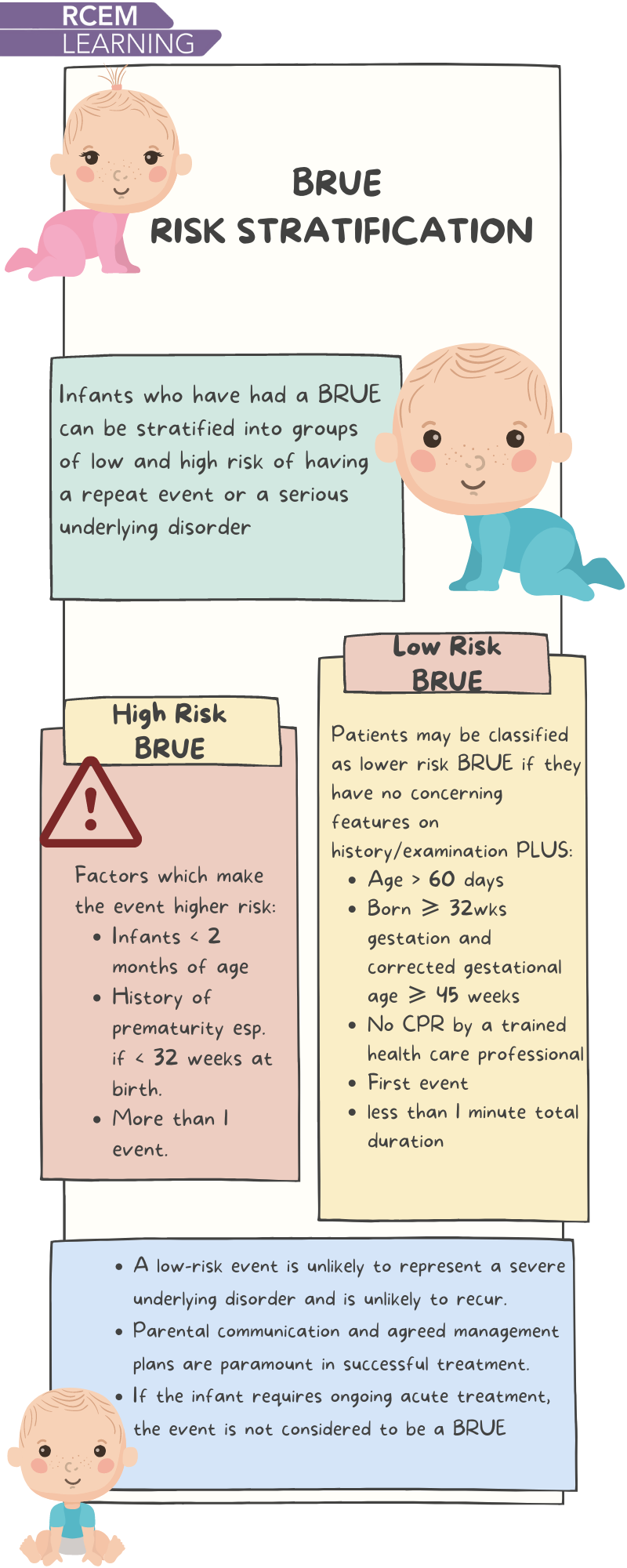
Low-risk BRUE:
High-risk → admit for monitoring ± targeted tests.
Corrected age = Chronological age − Weeks premature
Weeks premature = 40 − Gestational age at birth
Example:
24 weeks old, born at 28 weeks
Weeks premature = 12
Corrected age = 24 − 12 = 12 weeks → High-risk
Precision here distinguishes consultant-level candidates.
Avoid blanket septic screens and prolonged admission.
Exam tip: ECG is to evaluate QT; capillary gas screens metabolic causes.
SBA nuance: Suggesting CPR training may increase anxiety—use shared decision-making.
CriterionLow-RiskHigh-RiskAge | >60 days | <60 days
Gestation | ≥32 weeks | <32 weeks
Corrected Age | ≥45 weeks | <45 weeks
CPR (professional) | No | Yes
Duration | <1 min | >1 min
Recurrence | First event | Recurrent
Fail one criterion → high-risk pathway.
This guidance reflects paediatric emergency reasoning consistent with the Royal College of Emergency Medicine curriculum and learning objectives available via RCEMLearning.
Candidates should regularly review paediatric emergency modules on RCEMLearning to reinforce exam-aligned reasoning.
Whether preparing in the UK, Ireland, or the Middle East:
Disciplined reasoning—not defensive medicine—wins marks in the Final FRCEM SBA.
check our website for high quality frcem final sba questuibs regarding this topic here please : https://www.frcemstudyzone.co.uk/demo-quiz?category_id=7