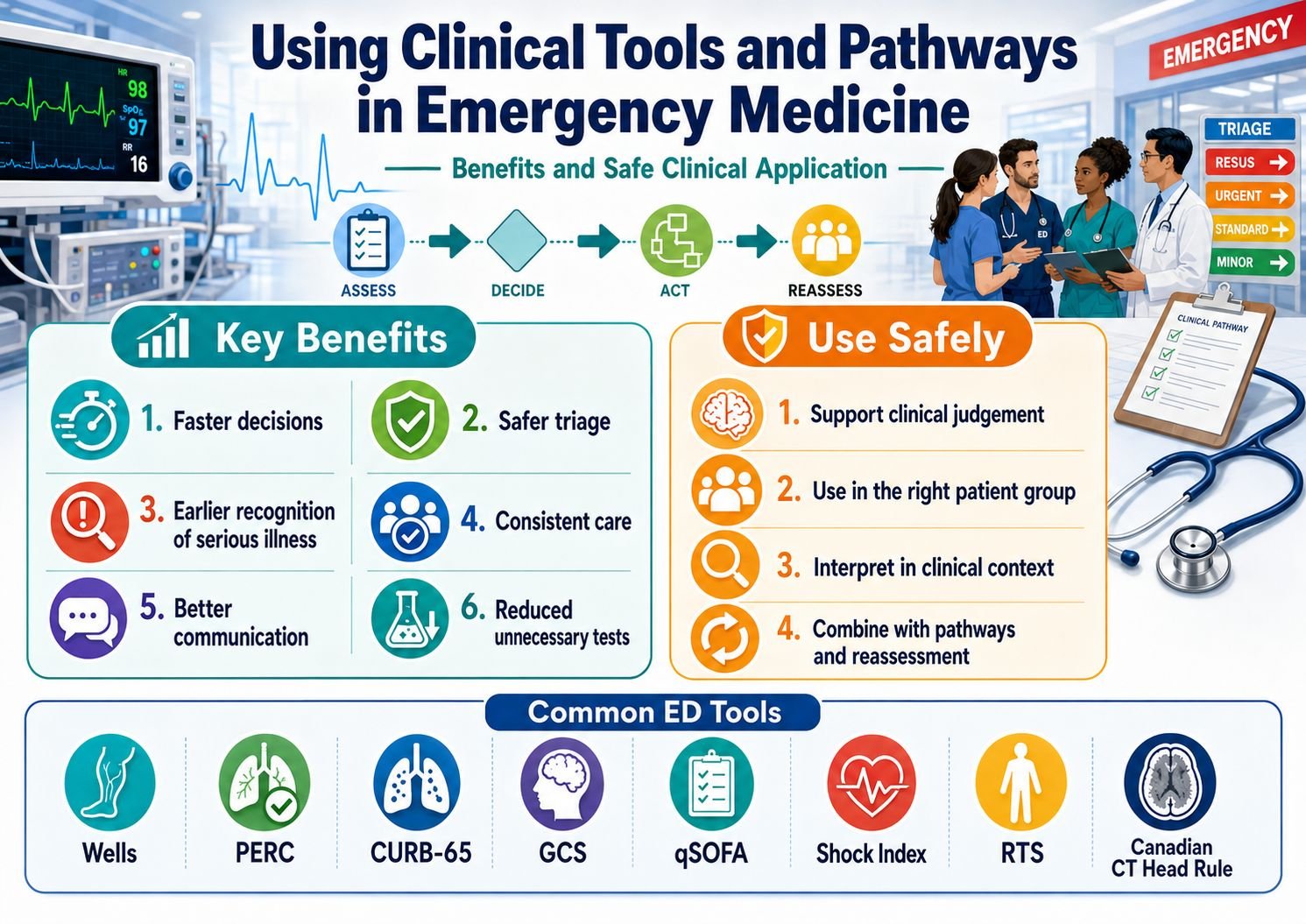
Emergency Medicine is a specialty built around rapid decision-making under pressure. Clinicians are often required to assess undifferentiated patients, identify life-threatening disease, start treatment early, and decide who needs admission, imaging, specialist referral or safe discharge.
Clinical tools and pathways are designed to support this process. They help structure thinking, reduce variation in care, and provide a safer framework for managing high-risk presentations.
Examples include:
These tools are not replacements for clinical judgement. Their value lies in helping clinicians make safer, more consistent and evidence-informed decisions.
The Emergency Department is a high-risk environment. Patients may present early in their illness, with incomplete information, atypical symptoms, or multiple competing diagnoses. Time pressure, interruptions and cognitive overload can increase the risk of error.
Clinical tools help by providing a structured approach. They convert key clinical findings into a reproducible decision framework.
For example, instead of relying only on general impression in a patient with possible pulmonary embolism, the Wells score helps estimate pre-test probability and guides whether D-dimer testing or CT pulmonary angiography is appropriate.
Similarly, CURB-65 helps assess pneumonia severity and supports decisions about admission, outpatient treatment or critical care escalation.
Clinical judgement is essential, but it can be affected by cognitive bias. Anchoring, premature closure, confirmation bias and over-reassurance from “normal-looking” observations are common risks in acute care.
Clinical tools act as a safeguard by forcing clinicians to consider specific variables.
For example, the Shock Index highlights the relationship between heart rate and systolic blood pressure. A heart rate of 110 and systolic blood pressure of 100 mmHg may not look alarming when viewed separately. However:
Shock Index = 110 ÷ 100 = 1.1
This is abnormal and suggests possible haemodynamic compromise.
The tool therefore helps identify physiological risk that might otherwise be underestimated.
Many emergency conditions are time-critical. Sepsis, major trauma, pulmonary embolism, acute coronary syndrome, intracranial injury and major haemorrhage can deteriorate rapidly.
Clinical pathways help clinicians recognise danger earlier.
Examples include:
The key advantage is that these tools encourage earlier action before obvious collapse occurs.
Without pathways, decision-making may vary significantly between clinicians, departments and shifts. This variation can lead to under-investigation in some patients and over-investigation in others.
Clinical pathways improve consistency by defining expected steps in assessment and management.
For example:
Standardisation is particularly valuable in busy departments, night shifts, handovers and multidisciplinary team care.
Scores and pathways provide a shared clinical language.
For example:
This allows rapid communication between ED clinicians, anaesthetics, intensive care, surgeons, radiology and medical teams.
A structured score can make escalation more objective and easier to justify.
Clinical tools can reduce unnecessary testing when used correctly.
For example, the PERC rule may help avoid D-dimer testing and CT pulmonary angiography in carefully selected very low-risk patients. Cervical spine decision rules may reduce unnecessary imaging in low-risk trauma patients. Head injury rules help identify patients who need CT while reducing unnecessary scanning in those at low risk.
This is important because over-investigation can cause harm through radiation exposure, false positives, incidental findings, unnecessary admission and patient anxiety.
The aim is not simply to do fewer tests. The aim is to perform the right test in the right patient at the right time.
For Emergency Medicine trainees and FRCEM candidates, clinical tools are high-yield because they link directly to real ED decision-making.
They help candidates understand:
For Final FRCEM SBA questions, these tools are commonly tested not as simple recall, but through clinical application. The candidate must decide when a score is appropriate, how to interpret it, and what action should follow.
The most important principle is that clinical tools support judgement; they do not replace it.
A low-risk score should not override genuine clinical concern.
For example, a patient may have a low score but still look seriously unwell. In that situation, further assessment, senior review, observation or investigation may still be necessary.
Conversely, a high score should prompt careful interpretation. If there is an obvious alternative diagnosis, the clinician should not blindly follow a pathway without reassessing the clinical picture.
Every clinical tool is validated in a specific patient group. Applying a score outside its intended population can produce misleading results.
For example:
Using a tool in the wrong context can create false reassurance or unnecessary escalation.
Some groups do not behave predictably.
These include:
For example, an elderly trauma patient may not mount a tachycardic response despite significant bleeding. A patient on beta-blockers may have a deceptively normal heart rate. A patient with dementia may not provide a reliable history.
In these groups, clinical judgement and senior review are especially important.
A score alone is not enough. The real value comes when the score is embedded into a clinical pathway.
A good pathway integrates:
For example, a sepsis pathway should not simply calculate qSOFA. It should guide lactate measurement, cultures, antibiotics, fluid therapy, reassessment and escalation.
A trauma pathway should not simply calculate RTS or Shock Index. It should support structured ABCDE assessment, haemorrhage control, imaging decisions, analgesia, senior review and transfer decisions.
When using a clinical tool, the clinician should ask:
The safest use of clinical tools is not mechanical calculation. It is thoughtful clinical application.
Clinical tools and pathways are essential in modern Emergency Medicine. They improve consistency, support early recognition of serious illness, reduce cognitive bias, improve communication and guide investigation and treatment decisions.
However, they must be used carefully. They are designed to support clinical judgement, not replace it. The best emergency clinicians use scores and pathways as part of a wider assessment that includes physiology, examination findings, comorbidity, trajectory, clinician concern and patient preference.
In Emergency Medicine, the safest approach is structured thinking combined with expert clinical judgement.
Clinical tools tell us what to consider.
Clinical judgement tells us what to do next.